"Since when do you speak Spanish, Viktoria?" I really don't but we'll get to that.
6:15AM
Getting up at 6:15 is just a bit early for my liking. Thankfully its bright out by 4AM otherwise getting up would be so much worse. I just kept telling myself its actually around 10 and time to get to the hospital. My body was not ready for breakfast though. I did force myself to eat a not so fresh banana though and headed over.
6:45AM
I got my lab coat filled up with books, stethoscope, notepads, iPhone and gum and headed to the ward. I was a bit early so I took the time to introduce myself to the nurses. Note to any med student: They can be your best friends or worst enemies but its ALWAYS good to have them on your side so try real hard so that they like you ;) One after another the doctors started showing up. Mostly guys, no surprise (2 of the 3 female doctors are at home with their new babies). In addition to myself, there are two more girls doing an elective in the department and a female intern (where are all the future male urologists at?). I decided to stick on the ward the first day to see what patients we have currently in treatment.
7:05AM
Dr.W, Dr.H and I did rounds on the two wards not part of the main ward. Nothing exciting to tell from that really. Since Dr.W had been on vacation the last 7 weeks and Dr.H just recently came to the department and the department recently got a new chief, my two doctors weren't quite sure when the morning meeting was taking place. They guessed 8AM. We didn't get through rounds and to the room until 8:12. We thought we were really cool because we were the first ones there. After about 2 minutes the chief walks in and tells us how cute we are sitting there because the meeting ended at about 8AM.....because it starts at 7:45. Oops.
8:15AM
Dr.W, an elective and I headed back to the ward and we discussed our current patients, treatment options, complications and further planning. Since it was a Monday, there wasn't a lot that needed to be done. The elective and I headed to the clinic to see if we could help out there.
9:00AM-1:45PM
Dr.M was in charge of the admissions for the day. We were allowed to head in and chat with the patients and get their history before he would join us, look over everything, discuss the upcoming procedures, get consent and send the patients up to the ward. We were in charge of getting their blood drawn and getting urine samples.
The four patients I worked with already nicely showed the variation in patients that show up in urology. Our youngest patient (already on the ward) was in his late 20s while the oldest one admitted by us today was a 81 year old female.
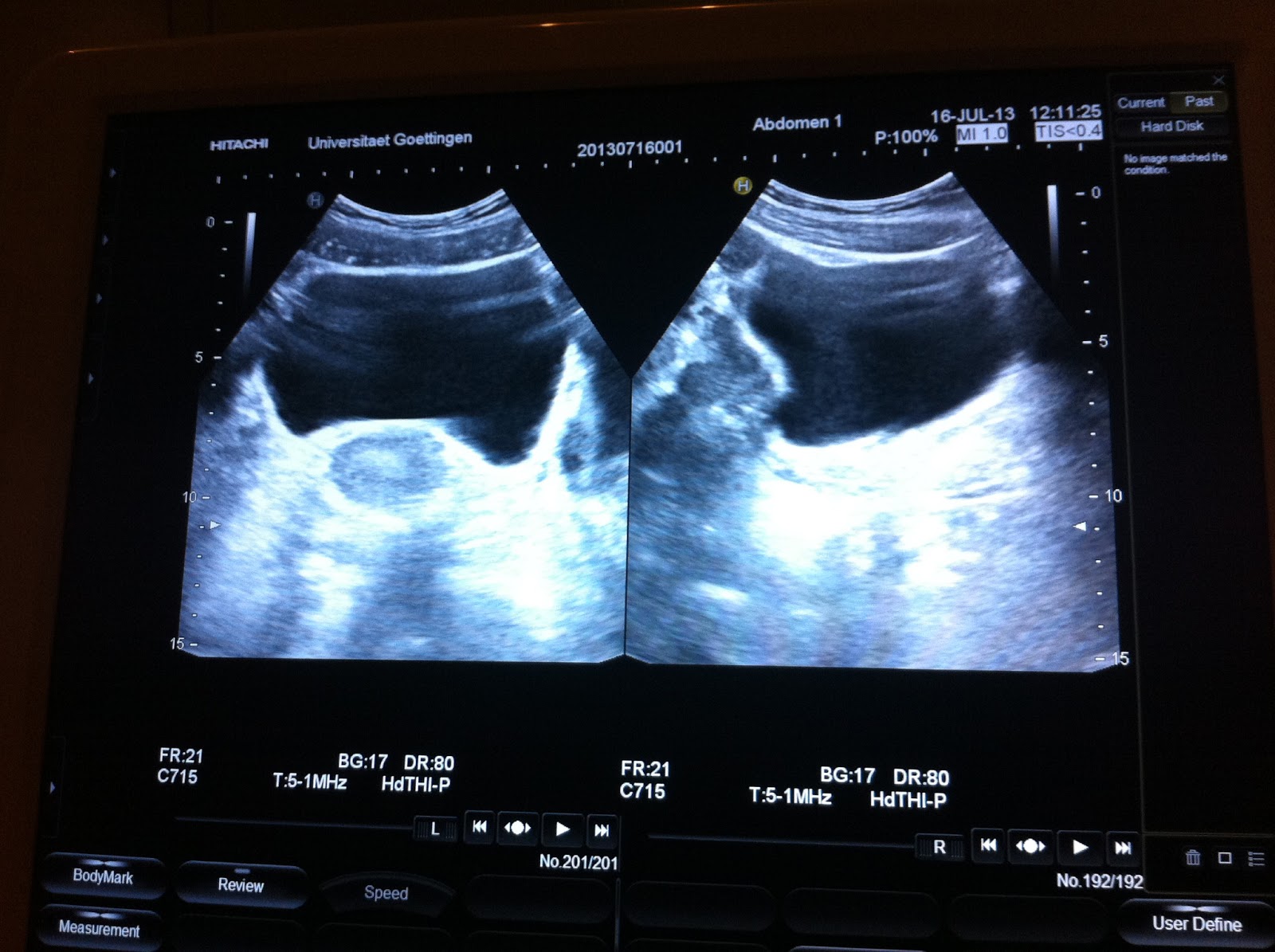
The cases included testicular cancer, kidney stones, varicoceles, kidney cancer and obstructions. We even ended up doing ultrasounds on the patients. I saw a patient with double kidneys on both sides, kind of bizarre! So although I wasn't in the OR today, it was a relaxed and informative day.
I'm always happy when I can use my English speaking abilities to help out in Germany. So when they told me the next patient only spoke English and Spanish I was excited and so where the nurses and doctors that I was there. Gosh dang it, why didn't I learn more from Mr.Wannicke back in High School?! I quickly looked up some Spanish words in case I'd need them. The standard: el testiculo, la vena, la arteria, los cojones (which is actually vulgar and was obviously not used with the patient) and so on because I was basically working with: si claro!, una cerveza por favor and vamos a la playa (all irrelevant for my case). Luckily the patient spoke English well enough that we could stick with that. We got all the work up done and then Dr.M joined us. Out of no where Dr.M starts speaking Spanish with the patient! I was flabbergasted! It wasn't fluent but it was a heck of a lot more than I had expected to hear out of his mouth! So with English, Spanish, German and hands and feet we explained the upcoming procedure to him and answered his questions. I even understood their conversation which just shows you that any little amount of foreign language can help out in unexpected situations! Stay in school and pay attention kids ;-)
After that I had to accompany my friend PKay to the ophthalmologist in Hannover so I had to leave early.
The other electives and I decided to split up the departments
clinic,
ward and
OR amongst ourselves during the weeks and rotate weekly or drop in and help if our respective department was running slow. I said I'd continue ward since I had started there this morning which unfortunately means being on ward every morning at 7 for rounds but since they are experiencing a bit of a summer break, I will try to get into the OR tomorrow as well.
On a side note: A thing I deal with basically every first day of an elective is my circulatory system. After months of just sitting in lecture to then sitting at my desk my body is not a fan of having to suddenly stand all day. Thus, the first few hours of my day are a roller coaster of feelings. Either I feel great or feel like I'm about to faint and no amount of water or pumping my muscles while standing can change it. I'll probably have the same phenomenon in the OR tomorrow with bright lights, multiple layers of clothing and face masks that make me think I'm getting less air.
It's an absolutely terrible few hours but after that I am good to go for the rest of the time. Basically I just want to make everyone aware of the fact that this is a completely normal thing! Most people are embarrassed by it and stand in the OR trying to keep it cool and the next second they are lying on the floor. No fun for anyone especially if there is a patient on the table because honestly
that person is more important than your dumb ass that didn't just say you need to sit down a second. I've had doctors from all levels insure me that it is totally normal and nothing to be ashamed of. Just thought I'd share that with y'all :)
And now for your urological entertainment. Meet the waving Eskimo.
We discovered him in our second semester during anatomy and in all reality he is actually a penis with cut open scrotum....you are welcome.
I'm off to bed, I'm spent.
Baci, V